

Currently Used Terms in Classification of Osteomyelitis
of the Jaws
Osteomyelitis
Acute / Subacute
While acute forms of osteomyelitis
can only be seen In common medical literature, most writers seldom identify the
type as an individual of their own these days.
Endurance past this arbitrary set time limit is then considered as
chronic osteomyelitis reflcting the inability the processes of host defense to
remove the liable the illness.
Osteomyelitis Recurrent The
recurrent osteomyelitis definition is unclear And confusing. And confusing.
There have been different disease mechanisms In some instances defined by this
one word, though Several lesion words describing the same object in other
instances have been allocated for
Chronic
osteomyelitis suppurative:
Chronic osteomyelitis suppurative
is also the choice word may can primarily be used in Anglo-American texts
interchangeably with the word
"secondary osteomyelitis," primarily used in literature Europe's
Mainland
Non-suppurative
chronic osteomyelitis
Therapy describes a term
"negative osteomyelitis" More persistent osteomyelitis community,
more heterogenic lacking fluid and fistula shape.
Osteomyelitis
Diffuse Sclerosing, Chronic youthful osteomyelitis:
One of the most confusing terms of
today's The nomenclature used for osteomyelitis is 'different sclerosing.
Osteomyelitis. The word seemed to
have contributed to In the medical literature, great confusion. A broad variety
of Denominations were used for this disease classification.
Chronic
Chronic, SAPHO Condition / Osteomyelitis multifocal (MORC)
a syndrome associated with synovitis, acne, pustulosis,
hyperostosis, and osteitis (SAPHO syndrome). Soon, several case reports and
studies were published, concluding a possible relationship between SAPHO
syndrome and DSO of the mandible
Ossificans
periostitis, Osteomyelitis Garrès
ossificans or ossifying
periostitis is strictly periodontal, Such a concise word as diffuse sclerosing
osteomyelitis for a condition caused by several similar conditions Entities.-Entities. It's just an inflammatory
periosteal response. to many unidentified triggers that contribute to training
of a new bone immature outside the normal
Layer of cortic [7].
In 95 % of cases, Staphylococcus aureus is a micro-organism, but a number of micro-organisms can be responsible for osteomyelitis(OM) . Other potential contamination routes consist in the proliferation from contiguous infection sources of open fractures with direct implantation and/or foreign body presence or postoperative instrumentation infection. Persistent OM frequently is related to systemic insufficiency contributing to chronic disability (e.g. due to the underlying diabetes mellitus). This manuscript focuses primarily on osteomyelitis hematogenic propagation.
The reach of this pictorial analysis is beyond more detailed discussions of the other ways of distribution. The nature of the blood supply depends on the patient 's age for diaphysis, metaphysis and epiphysis. A thorough understanding of the different patterns of OM among children and adults[8] allows for an understanding of different radiological patterns.
Although the growing plate has traditionally been regarded by a
specific age dependent vascularization as an obstacle for epiphyseal expansion
of infectious focus in children, this barrier is still permeable to magnetic
resonance imaging ( MRI), which is more susceptible to show subtle change in
the marrow as a sign of an early infection on the growth plate.
In extreme cases, Hunter's circulus articuli vasculosus primarily
spreads the virus that supplies the epiphysis. This can account for the unusual
incidence of osteomyelitis in epiphysical infancy [9].
CT offers excellent multiplanar axial image reconstruction, which
allows even the subtlest osseous changes to be delineated. CT shows abnormal
thickening of the affected cortical bone, with sclerotic alterations, medullary
cavity invasion and chronic draining sinus in chronic osteomyelitis. While CT
will display these differences before plain x-rays, because of reduced
soft-tissue contrast and sensitivity to ionizing radiation CT is less favorable
than MRI.
In osteomyelitis, the detection of sequestra in chronic
osteomyelitis plays a major role, since the osseous abnormalities surrounding
conventional radiography can mask these pieces of necrotic bone. The existence
of sequestered bone sections indicates the infectious process activity and
their identification is useful for guiding therapeutic options. For sequestra,
cloaca, involucra, or intra-osseous gas detection CT is superior to MRI and can
help in guide needle biopsy and joint aspiration; it is also useful in the case
of vertebral osteomyelitis[10].
For environments with a complex anatomy, computed tomography ( CT)
is useful for assessing recurrent osteomyelitis. CT may provide details on the
presence of sequestra, cloaca, cortical destruction and involucrum thickness.
CT is more exact than plain radiography and MRI, in particular in the
assessment of sequestrum formation. Moreover, the technique is useful for
imagery guided needle biopsy and microbiology aspiration material[11]. The use
of CT, however, should be carefully superior in children because of radiation
dose.
A common subtype, typically affecting the mandible but also in the
long bones, is Garré's sclerosing osteomyelitis. The main effects involve
children and young people. The etiology remains uncertain, since societies are
usually accused of being a harmful one. If the mandibular is affected, patients
have swelling , pain, and trismus. Images show that periosteum thickening is
important with the development of peripheral sensitive bones. Treatment of jaw
implication includes surgical tooth excision[12].
The occurrence and severity of mandibular osteomyelits, particularly soft tissue inflammation, are gradually examined with computed tomography. CT was not able to use osseous and soft tissue information at an early stage in the combination with high spatial resolution; however, CT was used only in patients with alleged osteomyelitis of the mandible after a latency. The CT findings in the acute process of osteomyelitis are an osteolysis region which is initially limited to the clogged bones. The cortical bone may be distorted and the focal mass can be demineralised. Further signs are smaller perforations to reach the subperiodic space .
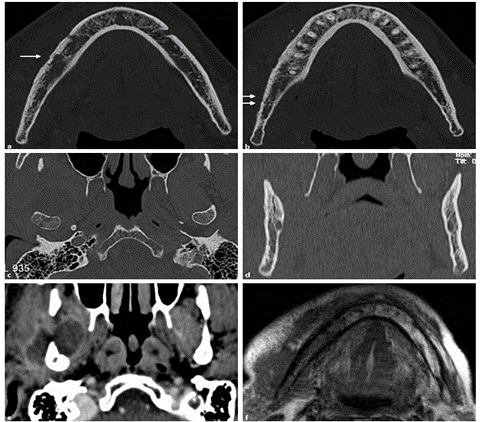
Extension normally takes place within the medullary cavity. The cardinal CT modifications that signify the presence of a recurrent stage of osteomyelitis are cancellous bone formation and cortical bone thickened through the endosteal and/or periosteal apposition. Additional findings may be calculated by a linear periosteal reaction and sequester formation. The CT secondary chronic osteomyelitis is a clinically suppurative condition of fistula and abscess development. Mixed sclerosis and osteolysis, sequester formation, and/or cortical bone fistulae (Fig . 2) consist of CT findings. The process from advanced stage acute to chronic osteomyelitis is a sequester formation. Due to the observation that the formation of secestors not only occurs in the chronic stage, but also in the late acute stage, the transition from acute osteomyelitis can be hypothesized probably before the arbitrary field limit of 4 weeks.
Another process involved the removal of a plate at the site of the lesion and the release of the lower alveolar nervous system and removal of the
lesion sub completely for collection for additional histopathological testing
of more representative material was taken [13].

completely for collection for additional histopathological testing
of more representative material was taken [13].
No comments:
Post a Comment