

In order to clarify the time and cost associated
with complex therapeutic treatment there is a desire for a good outcome
and long-term achievement. Life span in fixed prosthodontics is not just
reliant upon the accuracy and ability with which the work is performed, yet
additionally to a larger than usual degree upon a right evaluation and
analysis and in this way the usage and execution of proper design
principles.(1)Despite the publicity of dental implants, single crowns and
dental bridges are created on the known basis in ordinary practice. Therefore,
the research will discuss the complications additionally as causes and
kinds of most typical complexities associated with crowns, bridges,
implants and posts and cores.
Biological
complications
The
most familiar biological complication of all-ceramic crowns is loss of pulp
vitality. Another one is caries, which lead to dislodgment of crowns, and
many other conditions lead to the same result such as periodontitis and
abutment tooth fracture. It is said that in case of all-ceramic crowns,
the crowns become displaced due to dental caries have been 0.2%, 0% due to
periodontitis and 0.4% due to tooth fracture. For metal– ceramic crowns,
these figures had been greater and presented by 0.7%, 0.6%, and 0.9% respectively.
Therefore, the inference was that biological complications like caries,
periodontitis, and abutment teeth fracture had been greater in the
metal–ceramic crwons.From here, we can understand that the type of
restoration can affect the biologic health of teeth and oral tissues.
However, there is no considerable effect for the type
of fixation of the fixed prosthodontics (cemented or screw-retained) on
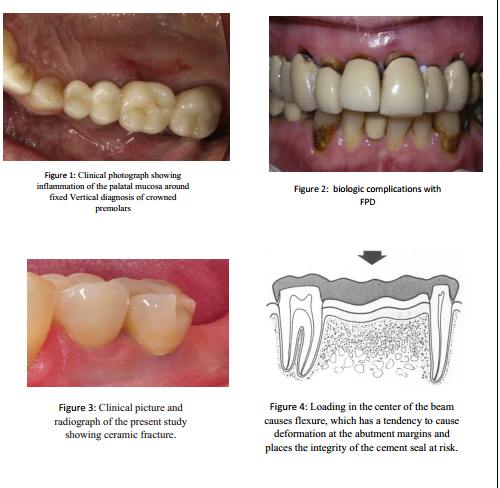
biological problems. There are clinical symptoms for biological failure of
crown restoration occur mostly in the form of inflammation either mucosa
inflammation or microsites (figure1). It can also lead to bleeding and
soft tissue discoloration around single crowns. (4) Periodontal
problems affect single crown by producing a clear distinction in the
plaque index, gingival index, and pocket depth.
(5)However, the presence of baseline condition decrease the percentage of
gingivitis. For resin bonded prosthesis, the effect of the prosthesis on
abutment teeth periodontal health used to be studied in 15 studies.(6) Seven
of the studies ) determined no periodontal troubles or no
multiplied incidence of periodontal disease while four reported the presence
of mild inflammation..So, the type of cement may affect the health of abutment
teeth periodontal ligaments.
Complications with FPD had been caries of abutment teeth, periapical lesions, pain/discomfort,
periodontal diseases and abutment fracture. This was showed after performing multiple
clinical examinations. (22), (23). (Figure 2) Peri‐implant mucosal
lesions have been mentioned in 10 researches. Two of them (24) used
the generic term ‘soft tissue complications’, other 4 suggested signs of
inflammation’
(25)gingival inflammation (26), gingivitis(Andersen et al. 2002) or
bleeding(Andersson et al. 1998a, 1998b) (27) stated on
‘periimplantitis’ which was described as probing pocket with a depth of ≥5
mm mixed with bleeding on probing or suppuration.Gotfredsen described cases with ‘soft
tissue dehiscence. The rest of researches (28) stated on fistula
formation. The most conventional biological complications for
implant‐supported SCs are peri‐implant mucosal lesions .This discovery was
explained with a clinical study based on evaluating the peri‐implant microflora
of implants in cemented and screw‐retained crowns(Keller et al. 1998). It used
to be concluded that the dental microflora has a significant effect on the
microbial colonization of the implants regardless the mode of fixation of
the crown.
Mechanical
complications:
Numerous entanglements happen because of the mechanical disappointment of the
fixed prosthodontics. One of these confusions is the fracture, which
mostly seen in porcelain crowns (Figure 3). Three studies recognized the
occurrence of porcelain crack with a mean pace of 3%.
(30), (31), (32) the explanation behind this can be referred to the sort
of maintenance. In later in vitro examinations, cement retained implant
upheld single MC crowns indicated estimations of crack opposition higher
than screw-held restorations. (33),(34),(35) The same number of
authors believe that the screw-access hole in screw-held restorations can
debilitate the porcelain around the opening and at the cusp tip, bringing about
porcelain fracture, while these that are cement held can conquer this
issue. (36), (37), (33), (38), (35), (39) Others state that neither
the area of the screw get to gap nor narrowing of the occlusal table had
any impact on the porcelain fracture resistance.
Fracture likewise was assessed according to crown
position in the arch and wear aspects/occlusal habits. Information with
respect to these two elements were accounted in an adequate number of
studies to be incorporated. The impact of five different elements (age, (43) gender, (40),
(41 ) etching/sort of cement, (40) finish line form, (42) and
ceramic thickness (42)) also were reported. Another thing that has a
marked effect on fracture resistance is the fixed prosthodontics metal
frameworks, which will flex when subjected to loading. Such flexure may cause
deformation near the abutment margins and place great stresses on the sealing
cement (figure 4). This may ultimately lead to disruption of the cement
layer and loss of cementation. Consequently, metal frameworks must be
sufficiently rigid to withstand such deformation. (43)In ceramo-metal
restorations deformation of the metal can lead to debonding and fracture of the porcelain;
hence, there is an added requirement for rigidity to provide more fracture
resistance. Precious metal (that is, gold-based) bridges had a
significantly longer mean service life than semi- or non-precious alloy
bridges. (44)
The failure for endodontically handled teeth used as
abutments is depended upon the type of restoration being supported and
therefore the degree of loading being experienced. An abutment for a
bridge is usually subjected to higher loading than a single crown abutment (49). Patients
with a tendency for parafunctional habit (for example, bruxism, clenching)
transmit stresses to their dentitions with higher frequency, higher
amplitude and longer period than normally experienced. Restorations in
these cases sufferers from being more liable to the problem of fracture. (50-52)
Morover, the abutment tooth must have the option to
offer great help for the extended bridge. This help to identify both the
measure of root and the measure of bond present hence determine the amount
of retention. A bridge replacing a maxillary canine is exposed to a bigger number
of worries than the mandibular since powers are transmitted outward (labially)
on the maxillary arch against the jaw (its most fragile point). At the
point when a cantilever pontic is utilized to substitute a missing tooth,
the powers applied to the pontic have a unique impact on the abutment
tooth. The pontic act as lever, which will in general be discouraged under
powers of occlusion. Spring cantilever spans gives a technique for
supporting a pontic at some good ways from the retainers. This sort of
abutment is both tooth and tissue supported. A gold bar, which fits in
contact with the palatal mucosa, associates the pontic to the retainer’s
consequently better retention. (58)
Perforation likewise is an extraordinary complexity
that have been noted particularly with fixed partial dentures. It might be
because of insufficient occlusal reduction , Insufficient occlusal
material , High forces in opposing dentition (plunger cusp) , Premature
contacts , contaminated metal or porosity in metal framework (subsurface,
back weight, draw back) .It may also result due to inappropriate
liquefying temperature , Improper example position , Improper sprue
(excessively slight) , improper area or parafunctional propensities . Twisting
of long range FPDs have been determined as an outcome of the use of thin
crown, delicate metal, absence of heat treatment, porosity in the metal,
bending of the metal foundation during the porcelain firing or utilizing
metal that is contaminated.(79)
Esthetic
complications
At the point when a good dental appearance is thought of, a few elements are of noteworthiness,
including tooth color, shape, position; restoration quality and the general game plan
of the dentition, particularly of the anterior teeth. Each factor might be
considered exclusively, but all parts together act in show to create the
last tasteful effect. However, many esthetic errors may occur during
fabricating a fixed prosthodontics. Failure to recognize esthetic expectation
of the patient, wrong shade determination, unnecessary metal thickness at
incisal and cervical area, Thick murky layer application, Surface botches
("chalky" appearance), Over glazing of the surface, Metal
introduction in connector, cervical and incisal insinuations, Dark space
in cervical third because of ill-advised pontic choice (Anterior), inability to
create incisal and proximal translucency, ill-advised contouring, Failure
to blend contra-sidelong tooth morphology, form, shading , position or
angulations .
Changing in the tooth shape is one of the most significant tasteful
complexities . The facial surface of the tooth is a piece of tooth structure.
It is definitive in molding tooth's appearance, especially when serious
changes happen in mature age. The incisal edge, which might be convex at
the beginning changes also as an outcome of abrasion and it, might in the long
time become concave. Cervical disintegrations and barely recognizable
differences between the clinical crown and the root which may result from
basic maturing or from oral cleanliness methodology should likewise be
considered.Morover, the issue of inappropriate gingival stylish is another
trouble. The morphology and measurement of supracrestal periodontal tissues are
the most significant parameters to be thought about in structuring a fixed
prosthesis.
The Esthetic Width and the supracrestal
connective tissue connection is resected during tooth planning so, tasteful
width should be regarded when structuring the prosthetic system and an
unmistakable space is essential between the coronal fringe of the gingiva
and the cervical edge of the system to give satisfactory space to the
fabrication of explicit shoulder porcelain. Shade selection failures are
very common in fixed prosthodontics. Until now, there is no deliberate
preparing on visual shade assurance for dental experts or dentists. (85-88)





No comments:
Post a Comment