

Teeth
assume a significant role in mastication, phonetics and esthetics. With ageing,
and because of various pathological factors like trauma, tooth lesions such as
caries as well as non-carious lesions, partial or total tooth tissue loss will
happen (2). Non-carious cervical lesions (cervical wear) are characterized as
the loss of tooth substance at the cement-enamel junction (Mair, 1992).
definitions also can be used to describe these cases such as ‘cervical
erosion/abrasion’ lesions and ‘abfractions (3). Dental caries is most regular
oral infectious disease. It is painful and caused by Streptococcus mutants,
acid and carbohydrates (4). If dental caries isn't treated, it will affect the
root of the teeth and finally uprooted the teeth. so, we need to detach the
caries at its early stage for avoiding surgical intervention. world health
organization has reported that 98% of adult people and (60_90) % of school
children have caries (5). Clinical appearance of Nonserious cervical lesions
can vary depending on the type and severity of the etiological factors involved
(6).
tooth surface loss, or tooth wear, is irreversible
loss of tooth. due to non caries reasons, that always produce destruction (Bassoon,
2012). TSL can be considered physiological or pathological (7). Numerous
factors are responsible to increase the growth rate of dental caries. these
factors are numerous as teeth condition, tooth. due and food habits. Dental
caries are predominantly two types (1): Enamel caries: this case of caries impacts
the enamel layer if it isn’t detected early it could spread to dentine and
reaches the root of the tooth Inter-proximal Caries: occur in position between
two teeth.
Dental caries:
A
deep carious lesion involves a greater depth of dentin, and its complete
removal can expand the problem of pulp exposure (13). Dental caries is a
critical global public health problem with substantial negative impacts.
Untreated caries among children can lead to disturbed eating and sleeping
habits, possible 5 hospitalization, diminished growth and reduced weight gain;
thus, seriously undermining their general health and quality of life (15). The
2 essential bacteria involved in caries formation are mutans streptococci and
lactobacilli (16). Aged persons are more affected by root caries due to
interaction of root with oral environment. this effect could be due to
physiologic retraction of gingiva or due to the harm of habits related to oral
hygiene and dental diseases treatment. In the United States and in Europe, the
prevalence of root caries is expanding as the populations are aging (16).
caries prevalence is affected by few factors that are difficult to control for,
including the dietary mineral substance (fluoride, calcium, and phosphorus),
health care, oral hygiene habits, and education level (16). The utilization of
fluoride to treat early carious lesions via remineralization has proven
effective. fluoride cause adsorption of calcium ions to affect enamel surface,
in addition to substitutes hydroxy ions to form fluorapatite, which has strong
acid resistance to demineralization (15). Poor oral hygiene conditions,
nutrition, and, particularly, avitaminosis, are portrayed in an early
publication as the reasons for a high rate of cervical caries among people who
utilize illicit drugs (14). Nanotechnology treats dental caries in two primary
approaches. In the first approach, the nanomaterials with fluoride and calcium
release ability such as calcium phosphate, calcium fluoride, hydroxyapatite and).
are utilized in a process calls remineralization. implementation of
antibacterial nanomaterials as, silver, quaternary ammonium polyethyleneimine
and zinc oxide nanoparticles is the second approaches (17). Examination of
ancient skulls shows that root caries was more frequent than coronal caries in
old humans (14). Examinations of the microhardness of the root surface show
that its decrease is greater in the inner than in the outer dentin.
Classification
of Non-Carious Lesions Due to Tooth Surface Loss:
the subsequent four categories are the general
classifications of tooth surface loss. However, in most cases, many of those
factors lead to tooth surface loss and poses diagnostic and etiological
challenges.
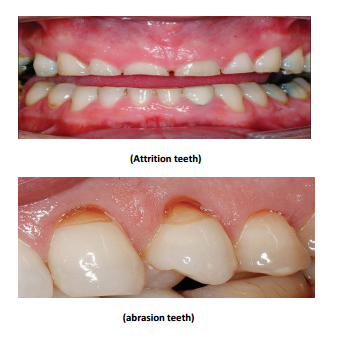
Attrition:
Attrition is that the physiological wearing a
way of dental hard tissues through tooth -to-tooth contact, without the
intercession of foreign substances (8). It should in principle occur by
two-body wear but mechanically it can't be differentiated sharply from dental
abrasion, since particles of enamel detached during attrition can act as
abrasive particles (2). During empty-mouth grinding movements, attrition can be
seen on the cusps and guiding surfaces as in parafunctional behaviors (i.e.,
bruxism). If the cause of attrition is involved, wear of the tooth is typically
seen as gleaming and well-defined facets (Kaydon’s, 2008) (7). the degree of
attrition depends on the applying coprocessor of lubricant available and
mineral content of the toot. It was recommended that dentine wear be greater at
lower loads due to its comparatively low mineral content, but that the fibrous
organic matrix help to minimize fracture at high loads, while the more
mineralized enamel will lose this mechanism (2). attrition can also cause
wearing of buccal and lingual surfaces, especially with especially surfaces.
Pathological levels of attrition of occlusal surfaces, beyond the limited
amount that is considered physiological, are related to parafunctional habits,
notably bruxism. However, excessive occlusal wear often seems to have a
multifactorial an etiology, so is discussed later, with regards to
communications of wear mechanisms (8). Proximal attrition (which occurs at
contact areas) can make a reduction of the dental arch (9).
Abfraction:
More recently, Grippe coined a relatively new
term 'abfraction' to represent the loss of dental tissues caused by
stress-induced non-carious lesions (2). Abfraction mean that “to break away”, a
name taken from the Latin word’s “ab”, or “away” and “fraction”. Abfraction
theory reports that dental flexure in the cervical area is caused by occlusal
compressive forces and tensile stresses, causing microfractures of the enamel
and dentin hydroxyapatite crystals with further fatigue and deformation of the
tooth structure (6). Abfraction lesions are seen at first on the buccal
surfaces and are typically wedge- or V-shaped lesions with clearly defined
internal and external angles (6). Abfraction are more prominent in adult people,
increasing from 3% to 17% between 20 years and 70 years (6).
Abfraction
means pathologic loss of hard tooth components because of biomechanical loading
forces; this loss is thought to be the result of flexure and chemical fatigue
degradation of enamel or dentin at some location distant from the point of loading.
Some reports mean that abfraction lesions are result of loading. Some and
frequency of forces (7). "Stanine et al" found that the loss of
tissue from bending forces of dentine beams was greater at pH 6 at pH 7, but
there was more wear on the compression surface of the beam than on the tension
surface and this relates to the abfraction hypothesis. (2). It is always
possible that experiments on extracted teeth are affected by pre-existing
cracks in the cervical enamel but these results cast doubt on the validity of
the abfraction hypothesis (2). Occlusal loading forces applied to the teeth are
transmitted through them to the periodontal supporting structures, which can
cushion and dissipate the resultant stresses. So that, mobile teeth are less
likely to develop the stress concentration that may lead to abfraction (9).
Abrasion:
Friction
between a tooth and an exogenous substance result in wear called “abrasion.” If
teeth are worn on their occlusal surfaces, incisal surfaces or both by friction
from the food bolus, this wear is called “masticatory abrasion” (9). 9 Abrasion
may occur because of overzealous toothbrushing, improper utilize of dental floss
and toothpicks, or detrimental oral habits for example chewing tobacco; biting
on hard objects as pens, pencils or pipe stems; opening hair pins with teeth;
and biting fingernails (9). Abrasive TSL can be observed on the occlusal
surfaces as a result of diet, the chewing of abrasive materials as tobacco or
continuous exposure to dust and grit (Turner and Missilries, 1984). It may also
be due to the consumption of vegetables which have not been washed properly and
thus still contain trace amounts of soil (LeVine et al., 2014). Other factors
such as pipe smoking, thread biting and holding of hair-pins between the teeth
can contribute to abrasion in the tooth surface involved (Chu et al., 2002,
Rath et al., 2017) (7). In the strict sense of the word, the term abrasion
refers to "wearing one surface against another by friction “.
Normal
tooth-cleaning practices produce some abrasion of tooth over a lifetime. In
tooth brushing abrasion, the toothbrush itself is just the delivery vehicle,
because brushing without paste has no effect on enamel and clinically little
effects on dentine (2). Some studies say that toothpaste has more relevance to
abrasion than does the toothbrush (Tonja et al., 2004a) (3). Clinically,
cervical abrasions in the cervical regions of facial surfaces of one or more
teeth are commonly seen as V-shaped notches. They are characterized by sharply
defined margins and smooth surfaces. although the general belief that cervical
abrasions are made by toothbrushes, toothpaste and brushing techniques, a
definite conclusion is so difficult to draw, as other factors such as erosion
and abfraction can also play an important role in the development of abrasion
lesions (Davies et al., 2002, Tonja et al., 2005) (7).
Erosion:
Dental erosion is characterized as the
pathological loss of hard dental tissue due to the chemical influence of
intrinsic or extrinsic acid without bacterial involvement (2). Dental erosion
is the loss of tooth structure by acid dissolution without the involvement of
bacteria. The acids can be intrinsic (regurgitated gastric acid) or extrinsic
(acidic industrial vapors or dietary components such as soft drinks, pickles,
acidic fruits) (8). Dental erosion is historically known as the dissolution of
the hard dental tissue caused by no bacteriogenic acids (Merman and ten Cate,
1996, Addy and Shelli’s, 2006). It has been reported that 29% of European
adults aged 18–35 years old showed signs of erosion (bio-corrosion), making it
a common clinical finding in this group (7). there are reports that poorly
chlorinated swimming pools with an acidic pH can make the erosion of dental enamel.
Other
factors like tooth enamel constitution and microenvironments within the oral
cavity in relation to fluid/food bolus movement can modify the susceptibility
of a given individual to erosion (2). Erosion, as defined by the American
Society for Testing and Materials Committee on Standards, is “the progressive
loss of a material from a solid surface because of mechanical interaction
between that surface and a fluid, a multicomponent fluid, impinging liquid or
solid particles (9). Erosion usually begins with the softening of the tooth
surface by acidic materials. When tooth enamel is presented to acid, it causes
loss of minerals from its superficial layer, which reaches out to a depth of a
few microns. The thickness of this softened layer ranges from 0.02 to 3 am (Lussa
et al., 2011). When the acid attacks and the softening process continues,
dissolution of the most superficial layer happen, and it is totally lost
(Barbour and Rees, 2006) (7). To offer chemical destruction of teeth, the word
'erosion' must be eliminated from the dental lexicon and replaced by the word
'corrosion' (9).
Discoloration:
dental discolorations are classified according
to the location and etiology of the stain. Extrinsic dental stain is found on
the surface of the tooth and has been subdivided into two categories: metallic
and non-metallic stain (10). The majority of tooth discolorations are extrinsic
in nature and appear as brown integuments (11). Yellow, green and orange
discolorations are made by chromogenic bacteria in bacterial plaque deposits in
connection with poor oral hygiene (Sutcliffe 1967). These discolorations are
most frequently found in children basically on the buccal surfaces of the
maxillary teeth (Leung 1950) (11).
Tooth
discoloration that outcomes from endodontic treatment is a typical aesthetic
problem in clinical dentistry. According to Nicholls the principal reasons of
intrinsic tooth discoloration related to endodontic treatment are decomposition
of necrotic pulp tissue, hemorrhage into the pulp cavity and endodontic drugs
and filling materials (12).
Conclusion:
Tooth
surface loss and the resulting non-carious lesions are issues that may be
difficult to properly diagnose and successfully treat. The etiology of the
tooth surface loss can be determined by examining the possible causes for each
patient and by observing the wear pattern, as the loss is shown in different
patterns and on different teeth surfaces for different types of tooth surface
loss (i.e., erosion, attrition, abrasion, and abfraction, or a combination) (2).
Tooth wearing is a universal result of ageing (Smith and Robb, 1996). Due to
the pathological levels of tooth wear, abrasion, attrition and erosion are
generally difficult to diagnose. (Smith and Knight, 1984). Therefore, choosing
different etiologies and making decisions based on hypotheses that suggest they
don't co-exist with each other is difficult. As with other types, cervical wear
lesions are possibly produced by a combination of erosion, abrasion and
attrition. There is strong support for the fact that erosion and abrasion are
very important in the development of wedge-shaped lesions along the cervical
teeth margins, but there is still insufficient evidence to confirm that
abfraction actually exists. There is a need for further research, especially
clinical, to establish the validity of the current abfraction as an entity.
There is much stronger evidence to suggest that cervical wear is a combination.
Illustrations:





No comments:
Post a Comment